quarta-feira, janeiro 25, 2006
$$$$$
Abbott sold $1 BILLION worth of Kaletra in 2005, worldwide -- a 12% increase over 2004.
BMS sold $696 Million worth of Reyataz in 2005, worldwide -- a 68% increase over 2004.
BMS claims that Reyataz has "achieved an estimated monthly new prescription share of the U.S. protease inhibitors market of approximately 28%."
Kaletra is now the 2nd antiretroviral to reach over $1 billion in sales -- GSK sold over $1 billion of Combivir in 2004 (they haven't reported 2005 financials yet). Gilead hasn't reported 2005 yet, either, but sales of Viread might also reach $1 billion.
Epidemia de sida na China é cada vez mais grave
A epidemia do vírus da SIDA na China é cada vez mais grave, alertou hoje em Pequim a Organização Mundial de Saúde (OMS), ao mesmo tempo que as autoridades chinesas anunciaram uma quebra no número de portadores do vírus no país.
"Que não haja confusão, a epidemia de SIDA-HIV está crescer", disse Hank Bekedam, representante da OMS na China, durante uma conferência de imprensa organizada pelo ministério da Saúde chinês e pela agência das Nações Unidas para a SIDA (UNAIDS).
As duas organizações anunciaram em conferência de imprensa que a China conta actualmente com 650.000 casos de seropositivos e portadores de VIH (Vírus da Imunodeficiência Humana), um número menor que as estimativas governamentais de 840.000, divulgadas em 2003.
Tanto os responsáveis governamentais, como os da UNAIDS e da OMS disseram, no entanto, que o menor número de casos de SIDA-HIV resulta de estimativas superiores à realidade no estudo de 2003 e não de um real decréscimo no número de pessoas infectadas.
"Com um número estimado de 70.000 casos por ano, a epidemia não demonstra sinais de abrandar", disse Hank Bekedam, que falou depois da apresentação dos números.
À margem da conferência de imprensa, funcionários do ministério da Saúde referiram que o número de novos casos de SIDA-HIV se situa entre os 60.000 e os 80.000.
"A aparente redução pode fazer alguns acreditar que a situação melhorou, mas isto não é verdade. A OMS receia mesmo que o número de infecções possa mesmo ser maior este ano", disse Bekedam.
O ministério da Saúde da China destinou em Dezembro 84,6 milhões de euros para o combate ao HIV-SIDA, a serem gastos em tratamento, testes e educação.
Segundo previsões da USAID divulgadas em 2005, sem medidas mais agressivas de combate à epidemia, o número de pessoas infectadas poderá atingir os 10 milhões de pessoas em 2010.
terça-feira, janeiro 24, 2006
O VIH em 3D

The 3D structure of the virus which causes Aids has been revealed for the first time, scientists say. The variable size and shape of HIV has made it hard to map, the team said in the journal Structure. So the UK-German team took hundreds of images of viruses, that are 60 times smaller than red blood cells, and used a computer programme to combine them.
Oxford University's Professor Stephen Fuller said the 3D map would assist in understanding how the virus grows.
(...)
Pfizer pára braço QD do maraviroc em naives
Comunicado da Pfizer:
January 24, 2006
DSMB Recommends continuation of maraviroc phase 3 development program
Treatment naive program continues with maraviroc twice daily dose;
Treatment-experienced program continues unchanged with once and twice daily dosing arms
Pfizer reported that the independent Data Safety Monitoring Board (DSMB) for maraviroc, Pfizer’s CCR5 antagonist in development for the treatment of HIV, met in January 2006 as part of their scheduled review of the phase 2b/3 development program. The maraviroc DSMB is an independent group of experts who specialize in the treatment of patients with HIV/AIDS and includes representatives from global regions where maraviroc studies are underway. The ongoing review of data by the DSMB helps to ensure the safety of patients participating in the studies.
The DSMB recommended that the three Phase 2b/3 clinical studies for the investigational drug in treatment-experienced patients continue as currently designed. They also recommended that Pfizer discontinue the maraviroc 300 mg once-daily dosing arm in the treatment-naïve program (Study A4001026), while continuing the other two arms of the study, maraviroc 300mg twice daily versus efavirenz 600mg once daily, unchanged. Both these agents are given in combination with zidovudine/lamivudine in this study.
This pre-specified analysis of Study A4001026 by the DSMB was put in place to ensure patient safety. It provided the DSMB with the opportunity to recommend discontinuation of a maraviroc treatment arm, should either fail to demonstrate non-inferiority to the efavirenz treatment arm. A review of the first 205 subjects treated for 16 weeks showed that maraviroc, given once daily at 300 mg in combination with zidovudine/lamivudine, failed to meet pre-specified non-inferiority criteria versus efavirenz plus zidovudine/lamivudine. The DSMB suggested that patients responding to the once-daily maraviroc combination should be offered the option of switching to twice-daily dosing of maraviroc.
Pfizer is informing all patients, investigators, ethics committees and regulatory authorities of this protocol change.
More than 1400 patients have enrolled in the maraviroc clinical development program to date. For more information about maraviroc clinical trials, please visit www.clinicaltrials.org
Médicos Sem Fronteiras passa para Governo moçambicano programa contra SIDA
A organização não governamental Médicos Sem Fronteiras (MSF) vai transferir para o governo moçambicano o programa de administração de medicamentos anti-retrovirais, que já beneficia 17 mil afectados pelo HIV/SIDA no país, disse hoje o coordenador do projecto.
Patrick Weiland referiu que os MSF estão a formar médicos, enfermeiros, parteiras e alguns activistas das zonas rurais de Moçambique para ajudar os doentes a manter o mesmo regime de tratamento.
Os MSF pretendem que a provisão dos medicamentos anti-retrovirais pelo sector público seja feita em fases, começando pelo centro de tratamento de HIV/Sida da província de Niassa, norte, onde assistem 380 pacientes por ano. "Discutimos a questão na semana passada em Lichinga (capital provincial de Niassa) e as pessoas entenderam que nós não podemos substituir o Ministério da Saúde", explicou Patrick Weiland.
"O facto de estar provado que certos modelos de tratamento anti-retroviral podem ser administrados por pessoas sem formação médica e com o envolvimento da comunidade também contribui para a decisão dos MSF", referiu. Entretanto, o programa desenvolvido de tratamento anti-SIDA em Maputo levará mais tempo para ser entregue às autoridades de Saúde de Moçambique, disse Weiland, sem avançar mais detalhes.
A taxa de seroprevalência em Moçambique ronda os 16,2 por cento na população adulta (dos 15 aos 49 anos), mas apenas 17 mil moçambicanos recebem tratamento anti-retroviral, dos 20 mil que necessitam do mesmo.
Desde 2001 que os programas de tratamento dos MSF na África Austral, nomeadamente no Malaui, têm surtido efeitos positivos por contar com a forte participação da comunidade, contrariamente ao que acontece em países ocidentais, destacou.
Ministro acredita que produção de vacinas vai permitir combater gripe das aves
O ministro da Saúde acredita que a produção de vacinas anti-gripais em Portugal vá permitir um efectivo combate ao vírus da gripe das aves se este passar a transmitir-se entre humanos.
Antes da apresentação do projecto de criação da primeira unidade de produção de vacinas anti-gripais em Portugal, no Parque Industrial de Condeixa (Coimbra), António Correia de Campos disse à Lusa que a capacidade que Portugal terá de produzir vacinas anti-virais e, em caso de uma pandemia, de vacinas contra a variante humana da gripe das aves, permitirá uma resposta a este problema que de outra forma não existiria.
"Em caso de uma pandemia de vírus da gripe das aves nos humanos, Portugal apenas poderia comprar as vacinas que sobrassem dos países produtores, o que poderia ser manifestamente insuficiente", disse o ministro. Segundo o ministro, a produção de vacinas anti-gripe é difícil e são poucos os países produtores de vacinas, pelo que estes têm prioridade na aquisição dos medicamentos que fabricam.
António Correia de Campos esclareceu que esta unidade irá produzir vacinas contra o vírus da gripe das aves nos humanos assim que o vírus (H5N1) adquirir a capacidade de se transmitir de humano para humano. Se isso acontecer, a produção será feita mediante um sistema de "corredor verde" mais acelerado e já aprovado pela Comissão Europeia com vista a uma melhor e mais rápida resposta perante um cenário epidémico.
Menos rápida será a produção de vacinas contra a gripe sazonal, a qual tem tido uma grande procura nos últimos tempos, em resultado dos receios da gripe das aves. O laboratório português Medinfar anunciou que pretende fabricar vacinas contra a forma humana da gripe das aves a partir de 2007 e abastecer 63 por cento do mercado nacional em vacinas da gripe sazonal em 2008.
A Medinfar estima poder começar a fabricar a vacina contra a gripe sazonal (que contém três estirpes diferentes de vírus inactivos, que são alterados anualmente de acordo com as recomendações da Organização Mundial da Saúde) no início do terceiro trimestre de 2008, de modo a estar disponível para a campanha de vacinação desse ano. Segundo o laboratório, deverá ser alcançada uma produção semanal de quarenta mil doses de vacinas contra a gripe sazonal, "o que permitirá, num período de oito meses, satisfazer aproximadamente 63 por cento das necessidades do mercado português".
Actualmente, a vacina contra a gripe sazonal é produzida apenas em nove países: Alemanha, Austrália, Canadá, Estados Unidos, França, Holanda, Itália, Japão e Reino Unido.
domingo, janeiro 22, 2006
Lá se foi a liderança política...

Le Radeaux de la Méduse, Théodore Géricault, 1819, Musée du Louvre
...na área do VIH/SIDA em Portugal.
Com um primeiro-ministro que não abre a boca sobre sida e um novo presidente de quem não se conhecem posições sobre a matéria, estamos bem entregues.
sábado, janeiro 21, 2006
Salas de Consumo: Razões e Objectivos
As salas de injecção assistida
Debate
20 de Janeiro de 2006
Aula Magna da Faculdade de Medicina do Porto
Serviço de Bioética e Ética Médica – FMUP
E Associação Portuguesa de Bioética
Salas de Consumo: Razões e Objectivos
Luís Mendão
Fundador da Soma Associação Portuguesa Anti-Proibicionista
Direcção do G.A.T. Grupo Português de Activistas sobre Tratamentos de VIH/SIDA
Comissão de promoção das salas de consumo assistido
Notas prévias
Quero, em primeiro lugar, agradecer o convite para um debate importante em que praticamente me fiz convidar.
Primeira nota polémica (?): o debate é essencial mas não pode servir, e em Portugal muitas vezes serve, para bloquear decisões e escolhas. A ética e o conhecimento têm que ser centrais no debate, processo de decisão e acção das políticas públicas e continuar centrais na avaliação, validação ou correcção das mesmas.
Pensamos que estamos no momento imediatamente anterior à decisão, que espero seja tomada, implementada, avaliada e corrigida em conformidade.
Segunda nota polémica (?): a participação da sociedade civil, através das organizações das pessoas afectadas pelos problemas deveria começar a ser norma nos processos de discussão, planeamento, implementação e avaliação das políticas públicas, não para se substituir ao conhecimento e aos decisores políticos mas contribuir com os seus saberes específicos, Esta participação tem também que ser exigente e deve servir para aumentar a capacidade das organizações não-governamentais para servirem eficazmente as suas comunidades.
Terceira nota polémica (?): Temos que aprender a viver com as drogas.
SOMA designa a droga (possivelmente o cogumelo amanita muscaria) consumida em rituais da antiga Índia, já citada nos Veda, os textos mais antigos da civilização indo-europeia.
É o símbolo da utilização ancestral de drogas e da sua integração cultural e social.
Na generalidade das comunidades, incluindo nas de tradição indo-europeia, registou-se, desde sempre, a utilização de substâncias psicoactivas, o que, muito frequentemente, foi factor da própria coesão social.
O alegado objectivo proibicionista de criar uma sociedade sem drogas é, antes de mais, contrário à compreensão histórica e ao que dela releva quanto ao conhecimento das comunidades e da condição humana. É, simultaneamente, pouco sério, pois a designação de droga, bem como a proibição que se lhe associa, não resulta apenas da avaliação farmacológica ou de apreciação de potenciais danos, mas é principalmente expressão de dogmatismo ideológico e jurídico.
Os resultados das políticas proibicionistas são expressão da ilusão em que os governos e as sociedades têm laborado. À sombra do proibicionismo, consolidou-se o poder económico, social e político do narcotráfico; soldou-se os seus interesses a relevantes actividades legais; provou-se o aumento exponencial do consumo clandestino de droga; propagaram-se algumas das mais graves epidemias contemporâneas: a sida, as hepatites víricas, a tuberculose.
O proibicionismo não só não atingiu, quer no plano nacional, quer no plano internacional, os seus objectivos declarados, como revelou ser, de facto, muito mais pernicioso do que os males que pretendia atingir. O desafio que se coloca é o de criar uma ordem social e política em que se reaprenda a viver com drogas. Trata-se, pensamos, de um empreendimento cívico, ético e civilizacional fundamental.
Introdução
Estratégias de redução de riscos: um imperativo ético.
A repressão e criminalização do uso de drogas foram claramente desenhadas com os objectivos de reduzir os problemas sociais e de saúde pública e individual resultantes do uso e dependência. O problema é que estas respostas simplesmente falharam os objectivos. Pior, em vez de resolver estes problemas, este modelo exacerbou problemas existentes e criou novos.
A proibição e criminalização caracterizou-se (e continua a caracterizar-se) por falhar os objectivos para que foi pensada e promovida como levou à exclusão social dos consumidores de drogas, à delapidação de recursos públicos limitados (hoje mais do que nunca), estimulou o crescimento exponencial do poder e riqueza de grupos de traficantes socialmente destrutivos e violentos e minou o estado de direito, a democracia, o sistema judicial e a saúde pública.
A adopção de uma ética de redução e riscos e de danos reconhece que a resposta proibicionista para o uso de drogas não funciona. A redução de risco não identifica a abstinência como condição para intervir. Mais consideramos não ético condicionar as respostas de públicas de saúde exigindo de um cidadão algo que este não está em condições física e mentais de fazer.
Tal dito, claro que consideramos que para algumas pessoas ou as mesmas pessoas em condições diferentes, a abstinência é um objectivo importante. Enquanto a proposta de redução de riscos não exclui a abstinência como objectivo, questionamos a noção durante muito tempo estabelecida que esta deveria ser a o único objectivo aceitável para qualquer política ou programa de drogas.
A ética da redução de riscos enfatiza o pragmatismo no modo de lidar com os problemas associados com o uso de drogas, por exemplo, em relação à utilização de tratamentos com opiáceos para substituir o uso de heroína clandestina, ou dar acesso a material de injecção estéril para reduzir a partilha de material contaminado e a incidência de infecções por via sanguínea. A prioridade é posta em manter vivos e sem infecções os que escolheram utilizar drogas, manter aberta a possibilidade de desabituação.
A moralização acerca do carácter intrinsecamente maléfico das drogas e do uso é evitado e reconhece-se que muitas das doenças e problemas associados ao uso resultam da resposta social vigente para lidar com o problema.
As salas de consumo seguro são um instrumento fundamental na estratégia de redução de riscos, por isso as nossas associações sentiram a necessidade de apoiar de forma organizada, de modo a exigir a concretização (e não ficar no rol imenso das declarações nunca passadas à prática), a declaração de 25 de Novembro de 2005, do presidente do Instituto da Droga e Toxicodependência, Dr. João Goulão, "Pretendemos instalar salas de injecção assistida em zonas onde esses consumos [de droga por via injectável] se efectuam em condições de extrema degradação” ao defender a instalação de salas de injecção assistida, nomeadamente em Lisboa e no Porto, como alternativa às "salas de chuto em cena aberta".
Salas de consumo: razões e objectivos
As salas de consumo são estruturas dos serviços de saúde criadas para promover e facilitar os contactos e a aproximação com populações específicas de consumidores de drogas em situações de grande risco sanitário, nomeadamente as que consumem drogas injectáveis na via pública.
As enormes carências de cuidados de saúde destas populações não podem ser resolvidas por outros serviços de saúde e constituem um problema para as comunidades locais que, como todos reconhecem, nem os programas sociais e de saúde, nem as polícias têm conseguido ou conseguirão resolver.
As salas de consumo, ou de injecção assistida pretendem dar resposta e resolução aos problemas destas populações e têm como principais objectivos:
1. Estabelecer pontos de contacto com as populações de utilizadores de drogas mais problemáticas;
2. Promover o acesso a serviços sociais, de saúde e tratamento de drogas;
3. Fornecer um ambiente seguro e higiénico para o consumo de droga a fim de reduzir:
- o consumo público de drogas e problemas sociais associados;
- a transmissão de VIH, hepatites e infecções bacterianas;
- a mortalidade e morbilidade associada às overdoses no consumo de drogas.
De acordo com a informação do Observatório Europeia da Droga e das Toxicodependências (OEDT) existem, na Europa, 73 salas de consumo em 40 cidades. A primeira abriu em 1986, em Berna, e a última em Oslo. Existem também salas de consumo no Canadá e na Austrália. Todas as avaliações reconhecem que atingem positivamente os seus objectivos. As salas de consumo seguro tiveram e ainda têm problemas, mas existe hoje suficiente conhecimento acumulado, boas práticas, recomendações e diferentes modelos adaptados a diferentes realidades, para evitar muitos deles.
A situação em Portugal, onde mais de 40.000 utilizadores problemáticos de drogas estão fora dos centros de tratamento e se registam, nos utilizadores de drogas injectáveis, as taxas mais altas da Europa de incidência e prevalência de VIH e Hepatites tornam urgente esta e outras medidas.
Compreendo que continuem dúvidas e perplexidades entre muitos mas penso que todos, os que com honestidade intelectual analisam a situação actual aceitam que temos que assumir decisões corajosas e que deixar tudo na mesma é inaceitável.
Sesimbra 19 de Janeiro de 2005, vinte anos depois de pela primeira vez ter defendido a urgência de criar salas de consumo
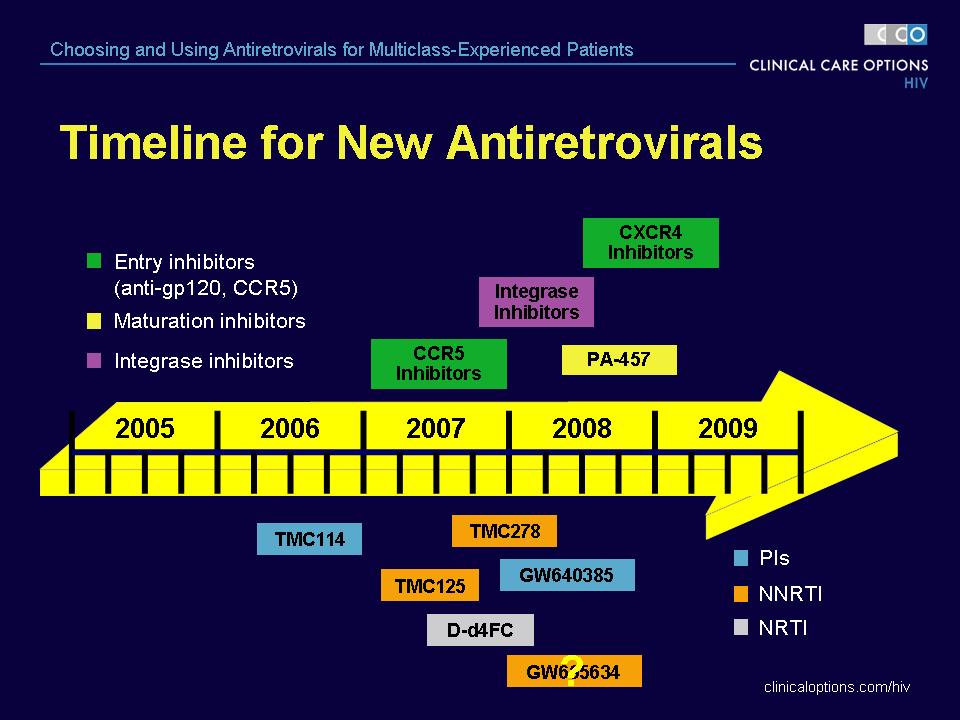
Pipeline ARVs
sexta-feira, janeiro 20, 2006
Acesso universal em 2010?!
19.01.06
Last week, UNAIDS and the UK's Department for International Development sponsored the first of three meetings of the Global Steering Committee of the Universal Access initiative, the "sequel" to WHO's 3x5 program, which sought to get 3 million people on antiretroviral treatment by the end of last year. The Universal Access initiative extends the promise of 3x5 targeting "universal" access to treatment, care and prevention, by 2010. (Well, we all should get busy if we're going to have heaven on earth in just four years' time!).
I attended the first meeting as a member of the committee with my community colleagues, Rodrigo Pascal from Chile, Susan Chong from Malaysia, Anandi Yuvaraj from India, Elizabeth Mataka from Zambia, Lillian Moreko from Uganda and Bob Vitillo from the faith-based organization, Caritas International (Raminta Stuikyte from Lithuania was unable to be there).
Let's say things did not start off well. The first night of the meeting began with a "working" dinner at which everyone in the group of about 30 people was to quickly say a few words about what they expected from the process. Much to my complete horror, the first up at the microphone was none other than garlic-toting, HIV-denying, treatment-hating, TAC-bashing, South African Health Minister Manto Tshabalala-Msimang, who proceeded to ramble on for about 15 minutes about how she was a nice person, but misunderstood, the glories of the South African AIDS response and the need to ensure that the response to AIDS is integrated into larger concerns around human development. I think the idea was to have Manto there to constructively engage the South African government, but it did another thing in my mind: it revealed the deep problems with UNAIDS' calls for the Universal Access initiative to be a "country-led" approach. This "country-led" approach was leading millions of people straight into the grave and no one, except a few of the community members in attendance, challenged a word she said that evening. I am not challenging the need to have an approach to scale-up that is driven by local needs and led by national goverments and civil society-I am challenging an approach that appeases the worst governments and gives them center stage and allows them to seize the agenda. For me, this was the Marie Antoinette moment of the AIDS epidemic-"let them eat garlic, African potato, olive oil and beetroot" instead of cake.
The second day of the meeting split up the participants into five groups: one on predictable and sustainable financing and macroeconomic constraints chaired by Manto and Peter Heller from the International Monetary Fund (please shoot me now I kept thinking, when these two problematic figures are leading this discussion!); the next on human resources capacity and health and social service system constraints chaired by the head of the Nigerian AIDS program, Babatunde Osotimehin and Sigrun Mogedal from Norway's development agency (who is an old-style health systems' advocate and sees scaling up ART as a potential threat to health systems development); the next on affordable commodities and low-cost technologies chaired by the French AIDS Ambassador Michel Kazatchkine and Minghui Ren, Deputy Director-General, China Ministry of Health (but with Merck's Jeff Sturchio among the small working group); the next on human rights, stigma and discrimination and gender equity chaired by Rodrigo Pascal and Edward Greene, Assistant Secretary-General of Caricom, the Caribbean Community; and finally, the last group on Targets and Milestones chaired by Anandi Yurvaraj and former US Ambassador to Uganda Jimmy Kolker from the US' PEPFAR program. Community members were split up between some of the groups, but Anandi, Susan and I were in the targets and milestones group, since it seems important to have targets and milestones for even small tasks, let alone something as grand as “universal access by 2010.”
Anandi, Susan and I were joined in the targets and milestones discussion by Jim Kim, the former head of the WHO’s HIV/AIDS Department (the incoming director, Kevin de Cock was not at the meeting nor was any senior WHO official), Debrework Zewdie from the World Bank, Paul DeLay from UNAIDS, and someone from the South African Ministry of Health. After a long and unconvincing discussion about why “global” targets such as the 3x5 goal were useful only one time in history, the conversation largely focused on the idea of selecting 5-10 key indicators on treatment, care and prevention, for which countries would develop interim 2008 and final 2010 targets—these targets would be developed by the end of 2006 and published and then aggregated for a set of “country-led” global targets. Let’s see how this idea fares in meetings #2 and #3 of the Global Steering Committee.
These working group discussions were short-only a few hours long and then everyone convened back into the larger group for report-backs. Sadly, much of what was said descended into vagueness. In the first working group on sustainable and predictable financing, there was no rallying cry for supporting the Global Fund nor any critique of the IMF and World Bank’s macroeconomic policies; in the group on affordable commodities, no one talked about the crisis around access to second-line therapies such as the new formulation of Kaletra and tenofovir or pediatric formulations or the failure of the current intellectual property framework under TRIPS to provide for any real way for countries to manufacture generic equivalents of pricey ARVs.
So, where are we? Well, we’re in deep shit.
It’s clear that the momentum for scaling-up access to treatment is dissipating. The Universal Access initiative wants to be all things to all people and will end up being nothing for millions infected with HIV/AIDS or at risk of contracting the virus. I’ve made my critique of the initiative in other emails, but the main fact is that without targets for treatment, care and prevention, with milestones, deadlines and consequences for inadequate performance, incentives for achievement, with detailed operational plans from the district level on up in each country, nothing is going to happen. The sad fact is that governments and the UN agencies that do their bidding are happy to let us die, most leaders like Manto have power and privilege that insulate them from the fate that falls upon the rest of their countrymen and women, most UN staff have cushy sinecures which they are unlikely to jeopardize by taking a risk, taking a stand for us.
All of this makes our work together more important than ever. We have to raise our voices locally, with our governments and demand access to treatment and prevention services, we have to hold our leaders accountable. We have to keep the pressure on the UN and donor governments. I’ve said this before, but we’ve got to treat this as a political campaign and fight to win. Right now, lots of us working internationally have tried to be technicians talking about policies on things from health systems, to diagnostics, to TB when we are in no position to get them adopted, or taken on the role of capacity-building again usually on technical subjects, doing trainings and workshops for our peers, when being in more meetings is the last thing we need to be doing. Lots of my work is just like this and my criticism starts with me. Why with all the wonderful people we work with can’t we create a powerful political movement to fight for our right to treatment? Part of our fate lies in ourselves and not in any external factors. In Nairobi, at a meeting of PWLHAs from around the world, we talked about radicalizing the AIDS movement, about conscientização, a critical awakening needed to free us from the NGO-ization, the domestication of our work. We need to have this conversation now, together, and move quickly. It means taking risks and perhaps taking directions that make us uncomfortable, giving up the security of the way we work now, the way we do business.
The UNAIDS/DFID meeting on universal access last week was a wake-up call for me. Access to AIDS treatment, in fact, even the larger fight against the epidemic, is in danger of being swallowed up and treated as just another intractable social ill. They’ve said AIDS needs to be de-exceptionalized, treated like other diseases, we’ve got to stop acting like there is a crisis, like there is something special about this virus that grips our bodies, and quietly jog like pigs to the market.
Well, not this pig. I won’t do it. Not ever.
Empresários portugueses e sida
A maioria dos empresários portugueses não está preocupada com o impacto do vírus da sida nos negócios nos próximos anos, apesar do ritmo de crescimento da doença. De acordo com os resultados de uma sondagem feita em 117 países, apenas 29 por cento dos inquiridos nacionais teme problemas, contra 71 por cento dos que estão crentes de que as empresas não vão ser afectadas.
No entanto, nem todo o mundo empresarial pensa da mesma forma. Segundo o inquérito realizado pelo World Economic Forum (WEF), 46 por cento dos cerca de onze mil directores de empresas contactados temem que a doença possa vir a ter um reflexo negativo nas suas operações futuras. Um aumento de nove pontos percentuais em relação ao ano anterior.
Apesar da preocupação, o relatório conclui que poucas são as empresas que fizeram uma análise dos riscos (9 por cento) e reforça a necessidade de uma alteração na política das empresas quando em causa está o HIV. Para isso, aponta a necessidade de minimizar o estigma e a discriminação, melhorar a assistência aos empregados doentes e apostar na prevenção.
“Para conseguir reunir com sucesso esforços contra a pandemia de HIV/sida, as empresas precisam de desenvolver programas de trabalho nesta área”, explicou Francesca Boldrini, directora da Global Health Initiative do WEF.
Entre nós, e de acordo com o mesmo relatório, 76 por cento das empresas inquiridas não tem uma política nesta área. Algo que não surpreende Francisco Porto Ribeiro, da Associação Abraço. “Em Portugal, aposta-se na técnica da avestruz, no esconder a cabeça.” Por isso, as respostas das empresas aos contactos feitos pela Abraço para acções de prevenção têm sido, na grande maioria, negativas. “Dizem que é uma perda de tempo, que não conhecem casos, o que revela uma falta de interesse e pouca clareza.”
RECEIOS COMEÇAM A CHEGAR CÁ
“Há motivos de preocupação de uma forma geral”, refere Caldeira Santos, coordenador do programa Solidariedade da Associação Industrial Portuguesa (AIP). Apesar de não ter, até ao momento, uma política destinada exclusivamente à prevenção da sida, em 2000 a AIP lançou um programa de apoio [!!!] aos trabalhadores que inclui a realização de testes de despistagem de consumo de álcool e drogas.
“A ideia não é castigar o trabalhador, mas procurar recuperá-lo”, confirma. Um programa que contempla ainda sessões de esclarecimento e seminários, nos quais o tema sida é também abordado. Um trabalho que, segundo Caldeira Santos, só existe se a direcção das empresas estiver desperta para o problema.
COMPORTAMENTO DOS PORTUGUESES
Há três comportamentos que associados evitam o contágio de doenças sexualmente transmissíveis. São eles: informação; motivação para prevenção; e saber fazê-lo. Conclusões de um estudo dirigido por Américo Baptista e que é hoje apresentado no IV Simpósio da Universidade sobre educação sexual, até sábado. O relatório faz parte de um projecto internacional onde o conhecimento e os comportamentos das pessoas, face a este problema, são analisados.
Em Portugal, nos homens, ter ou não ter conhecimento não está relacionado com as práticas de risco. Nas mulheres, quem tem mais informação também é quem mais está associado a actos de risco. Isto implica que os homens contaminam mais que as mulheres.
Brasil e Argentina colaboram para produzir ARVs
Argentina-Brazil to team up on AIDS
BUENOS AIRES, Jan. 18 (UPI) -- Brazil and Argentina will collaborate on a project to produce anti-AIDS drugs in efforts to reduce the price of treatment, Argentine officials said Wednesday.
The Argentine Interior Ministry said a plant to produce the drugs could be constructed in Argentina at a cost of $10 million. The decision was announced the same day Argentine President Nestor Kirchner met with his Brazilian counterpart Luiz Inacio Lula da Silva in Brasilia.
Brazil has already made significant inroads into the treatment of patients with HIV and AIDS, providing free medication and prompting pharmaceutical companies to lower prices, by threatening to break patents and producing generic version of the drugs.
IDT acredita ser possível planear criação de "salas de chuto"
| O presidente do Instituto das Drogas e da Toxicodependência (IDT) garantiu hoje que há abertura por parte do Governo para criar "salas de chuto", considerando ser possível programar a sua execução ainda este ano. |
Na sua opinião, as salas de injecção assistida devem começar por ser implementadas enquanto experiência-piloto em Lisboa e no Porto, grandes cidades "sedes dos grandes problemas ao nível da desinserção e da degradação da população toxicodependente".
João Goulão entende as salas de injecção assistida como "uma porta de entrada para um sistema de tratamento", afirmando que a criação das mesmas deve ser sempre entendida no âmbito da redução de danos.
Considerando a sua criação "útil", o responsável acrescentou que a sua concretização apenas depende da vontade política do Governo.
"Há enquadramento legislativo que permite a sua criação, apenas falta o pontapé de saída que será desencadeado na sequência de uma manifestação clara de vontade política", disse.
O presidente do IDT justificou a abertura do Governo relativamente a esta matéria com o facto da criação de "salas de chuto" estar consagrada no plano nacional contra a droga e toxicodependência, que se encontra em fase final de aprovação.
"Há abertura do Governo, desde logo ao assumir o plano e assumir também que os caminhos apontados na estratégia de 1999 se mantêm actuais", sustentou João Goulão.
Contudo, o responsável salientou que a criação de salas de injecção assistida dependem muito dos meios financeiros disponíveis e dos diagnósticos territoriais.
Para o presidente do IDT, terá que existir um diagnóstico "tão consensualizado quanto possível" relativamente à criação destes dispositivos.
João Goulão entende que as entidades que operam no terreno - autarquias, organismos da administração pública e organizações não-governamentais, além do próprio IDT - terão que se pronunciar sobre o assunto e apontar quais as prioridades para o combate à droga.
Quanto aos meios financeiros disponíveis, se apenas for permitido criar mais um centro de atendimento a toxicodependentes em alternativa a uma sala de consumo assistido, João Goulão admitiu escolher a primeira opção.
A sala de injecção assistida "só faz sentido integrada numa rede alargada de dispositivos de redução de danos", frisou.
Quanto à instalação destes dispositivos nos estabelecimentos prisionais, João Goulão afirmou crer que há condições para que durante este ano também haja uma decisão a este nível.
As igrejas de Dublim
By Bob Huff
There is something Old World about the biannual European AIDS Conference. The
two I have attended were held in cold, northern towns where fuels like peat and
coal are still used to heat rooms. This year's meeting, in Dublin, Ireland, was
sponsored by the European AIDS Clinical Society (EACS) and offered two full
days of scientific talks and poster presentations to doctors and researchers
from around the continent. But unlike the Annual Retrovirus Conference in the
US, which primarily attracts scientists and physicians with a strong interest
in research, the European conference is also attended by a substantial number
of everyday, working clinicians who come to get a refresher course in
state-of-the-art HIV care.
As at most medical conferences, outside of the hushed meeting rooms more festive
attractions await, including a forest of posters and a colorful exhibition hall
where pharmaceutical companies set up tents to woo doctors who wander into
camp. This is the village marketplace, a swirling festival of lights and video
screens where the throng mingles beneath giant logos amid laughter and the hiss
of espresso makers.
At EACS, though, more than any conference I've been to, it is the pharmaceutical
company-sponsored satellite session that seems to be the central attraction. Not
exactly an official part of the scientific program, satellite sessions are
granted to the drug makers in return for significant financial support of the
conference. Not surprisingly the companies use these events to feature their
latest products and to promote recent data that has appeared in proper science
sessions. In Dublin, nine companies held satellite sessions over a three day
span, beginning at 7:30 in the morning and ending well after dark.
These sessions began to feel a bit like church services, packed with pilgrims
come to witness eminent doctors uphold enduring truths and argue the nuances of
contending theologies. In honor of the tenth anniversary of the advent of truly
effective HIV treatment, almost every company's satellite presentation began
with a ritual recitation of the miracle of HAART. In Dublin we gathered to hear
the ancient faith affirmed: "The goal of antiretroviral therapy is to achieve
maximum virologic suppression."
They Love to Tell the Story
The Concert Hall of the Royal Dublin Society has a reverential air to it, made a
bit musty by shelves of thick Gaelic books that line the hall. At nearly every
session a hushed congregation fills the great room, rising to the rafters and
spilling into the nave aisles. Onstage, sponsors' crusade banners flank a large
central screen that displays an endless procession of PowerPoint slides. The
high priests of European AIDS medicine preside over these sessions and bid for
the hearts of the multitude with impeccably reasoned logic that leads from
point-to-point and slide-to-slide, arriving at a version of truth the sponsors
hope will prove undeniable. Their presentations are as finely honed as a
Jesuit's tract. Often they are scripted by third-party medical communications
firms, and the presenters are well compensated for their aura and expertise.
The arguments are crafted to lead - not push - the learned audience to the
desired epiphany. But free will is respected and the audience is never bullied
and rarely cajoled, although sometimes in the hands of a less skilled presenter
the pitch becomes too obvious and clangs like a cracked bell.
The topics of these sessions are like parables that reveal the patron's
underlying message. If the theme is lipoatrophy and how to avoid it, you know
you are in the church of Gilead to learn about the demons of thymidine analog
NRTIs. The sermon is subtle and you may hear the virtues of Viread invoked only
once or twice during the hour; yet to those with eyes that can see, the path is
clear: Truvada will set you free. If the devil is lurking in the lipids, then
this morality play is about the evil Kaletra, and rescue by good King Reyataz
or Sir Viramune is certain. But if you are called to worship time and tradition
by the old sage Abbott, then it's mighty Kaletra reciting the ancient mystery of
virologic failure without PI resistance.
In a kind of communion ritual, attendees sometimes receive small devices that
allow them to register their opinions on formal questions posed by the
presenters. Within seconds the collective responses are displayed on the big
screen for all to behold and wonder at. In these moments the secret heart of
the congregation is revealed. Often responses seem preordained, such as when a
question points to an obvious choice that reinforces the sponsor's message.
This is a pedagogic exercise and seems very effective. But the beliefs of the
mob can be frightening too. In a catechism sponsored by the makers of efavirenz
(Sustiva, Stocrin), the limits and dangers of nevirapine were drilled
unmercifully, yet a sizeable minority of respondents never quite seemed to
grasp that they risked a case of liver failure by prescribing nevirapine to a
woman with more than 250 T cells (over 400 for men).
These errant answers are a sobering reminder of why satellite sessions are so
useful. Despite how complex treating HIV can be in day-to-day practice, the dos
and don'ts must be made sufficiently simple so that garden variety doctors - the
parish priests of medicine - can keep the message straight and tend their flocks
without losing any sheep to the wolves of toxicity, resistance, or
lipodystrophy. When the guidelines are made clear, adherence to the faith is
more likely.
There were no apostates or freethinkers in the big hall. No heretics hailing
hydroxyurea, immune modulation, or other theories that stray from the central
doctrine of everlasting viral suppression. Although Merck allowed a peak behind
the veil to suggest a coming paradise of therapeutic vaccines and integrase
inhibitors, most companies offered redemption here on earth, available now (or
soon) at your local pharmacy. The sponsors' prize for mounting this pageant is
a buttressed position in the minds of Europe's doctors - and a possible up-tick
in market share. The doctors get a renewed awareness of the complexities of
treating HIV and some measure of comfort knowing they are in touch with the
mainstream.
quinta-feira, janeiro 19, 2006
Estudo coloca dúvidas sobre eficácia do Tamiflu em caso de pandemia
Público 19.01.06
Um estudo de investigadores italianos põe em causa a eficácia do medicamento Tamiflu no caso de uma pandemia de gripe das aves entre os humanos e afirma mesmo que não há qualquer produto no mercado que fosse eficaz.
Até agora, o Tamiflu (nome comercial da substância activa oseltamivir) é considerado um dos poucos antivirais eficazes no tratamento dos pacientes com gripe das aves, o que levou os governos europeus e dos Estados Unidos a armazenarem reservas desse medicamento para o caso de uma pandemia.
Mas o novo estudo, hoje publicado pela revista médica britânica "The Lancet", da responsabilidade do instituto de investigação italiano Cochrane Vaccines Field e financiado em parte pelo Ministério da Saúde britânico, considera que nenhum dos medicamentos existentes teria grande eficácia. Os autores do estudo analisaram outros medicamentos contra a gripe, como o Relenza, semelhante ao Tamiflu, a Amantadina e a Rimantadina.
O chefe da equipa de investigadores, Tom Jefferson, diz que até agora nem o Tamiflu nem o Relenza reduziram a mortalidade entre os poucos doentes com gripe das aves a quem foram administrados. "Sou membro da raça humana e espero que sejam eficazes, mas confiar num único remédio é um suicídio", afirmou.
Além disso, os cientistas advertem que não se poderá travar uma potencial pandemia de gripe das aves apenas com medicamentos. O uso de antivirais não deve impedir a adopção de outras medidas mais úteis de saúde pública, como a higiene e o isolamento para conter a expansão da doença.
Mas o Ministério da Saúde britânico, que decidiu armazenar 14,6 milhões de doses de Tamiflu e que financiou em parte o estudo, acrescentou hoje que "pode ser enganoso" afirmar que este medicamento não são eficazes contra a gripe das aves. "A nossa estratégia antiviral está em revisão constante e estamos a examinar alternativas complementares", indica ainda.
quarta-feira, janeiro 18, 2006
Estudo SMART descontinuado II
Treatment Action Group Statement on the Termination of the SMART Study
New York NY, January 18, 2006 – The Treatment Action Group (TAG) today expressed disappointment that SMART – a large, international study comparing CD4-guided, intermittent antiretroviral therapy to continuous treatment – has had to be stopped due to a significantly higher incidence of clinical events in the intermittent treatment arm. TAG salutes the many researchers and participants involved in this large and important trial of HIV treatment strategies. However, TAG also wishes to stress that the conclusion being promulgated by the National Institutes for Allergy & Infectious Diseases (NIAID), “International HIV/AIDS Trial Finds Continuous Antiretroviral Therapy Superior to Episodic Therapy” (see http://www.nih.gov/news/pr/jan2006/niaid-18.htm), could be over-interpreted. SMART has shown that, over the short term, continuous therapy is superior to the specific strategy of episodic therapy employed in the trial.
SMART evaluated a “drug conservation” approach that involved interrupting therapy when CD4 counts crested 350 cells and restarting when they fell below 250, and compared this to a standard “virological suppression” strategy using continuous therapy. The primary endpoints were progression to AIDS and death in the two arms, with secondary endpoints including incidence of potentially drug-related toxicities such as cardiovascular disease and liver problems. The study was addressing an important question because, while it is known that continuous therapy is beneficial in the short term, it remains unknown whether there is a point at which long term toxicities become a greater risk than events related to disease progression. It is also not known if intermittent CD4-guided therapy might be a less costly and toxic strategy for preventing disease progression. The study has reportedly been stopped by the Data Safety Monitoring Board (DSMB) due to roughly twice as many clinical events occurring in the drug conservation arm compared to the virological suppression arm. The nature and seriousness of the clinical events in question remain unknown at this time. Perhaps surprisingly, it is also reported that there was a higher incidence of events relating to drug toxicity in the drug conservation arm.
It is important to emphasize that the cessation of SMART does not necessarily mean that all treatment strategies involving interruptions of antiretroviral therapy are dangerous, just that the specific approach employed by the SMART study design was less successful at preventing clinical events than continuous treatment. There is a large body of data suggesting that individuals who initiate therapy with relatively high CD4 counts (for whom therapy would no longer recommended based on recent guidelines) can safely interrupt therapy.
Previous treatment interruption studies have also uniformly identified the CD4 nadir (lowest ever CD4 count, usually experienced before any antiretroviral therapy was initiated, or after virologic treatment failure) as a predictor of clinical events during treatment interruption and the SMART study accepted participants without regard to their CD4 nadir.
One of the key goals of the SMART study was to answer the question of whether less exposure to antiretroviral therapy would reduce the incidence of potentially life-threatening drug-associated toxicities. Recent data has emphasized the importance of addressing this question, suggesting that such toxicities can pose a greater risk for individuals on therapy than clinical events related to disease progression (see Reisler et al, JAIDS 34;4:379-386, 2003). In light of this fact, TAG strongly believes that further studies of treatment interruption and intermittent therapy strategies, addressing questions different from those addressed by SMART, continue to be warranted. Data from the SMART study should be used to design potentially safer approaches to CD4-guided therapy, with particular attention paid to the impact of CD4 nadir and the CD4 threshold for restarting therapy on the outcome of SMART. Ongoing trials of treatment interruption strategies, such as the international DART trial, should be reviewed in order to establish whether the data from SMART impacts the study design, but it would be premature to cease all investigation of intermittent treatment strategies because of the results from SMART.
The early cessation of SMART also means that the long term incidence of toxicity-related events among individuals on continuous antiretroviral therapy in this study will not be quantified unless follow-up is continued. TAG urges to the study sponsors to follow-up study participants for long term outcomes.
The SMART study was designed and conducted by the Community Programs for Clinical Research on AIDS (CPCRA), an international network of clinical trial sites funded by the Division of AIDS (DAIDS) of the National Institute of Allergy and Infectious Diseases (NIAID), one of the National Institutes of Health (NIH). TAG has been a strong supporter of the SMART study and believes that it asked and answered a question of paramount importance in the search for optimal antiretroviral treatment strategies, balancing the need to preserve immune function with that of avoiding unnecessary toxicity and expense.
Well designed studies that ask and answer important questions in a reliable, definitive way with adequate sample size, statistical power, participant retention, and length of follow-up are all too rare in the HIV field. The NIH should be commended for supporting, and the CPCRA for designing and executing this important study, which adds to our understanding of the optimal ART standard of care.
http://www.treatmentactiongroup.org/
UNESCO firma acordo com grupo de multinacionais para lutar contra a SIDA
A UNESCO assinou em Paris um acordo de parceria com um grupo de empresas multinacionais para reforçar a luta contra a SIDA nos próximos cinco anos, até 2010, anunciou a agência das ONU para a educação, ciência e cultura.
O acordo foi assinado pelo director-geral da agência, Koichiro Matsuura, e o presidente da Coligação Mundial das empresas contra a SIDA, Richard Holbrooke, ex-secretário de Estado adjunto dos EUA para a Europa.
A iniciativa pretende alargar a mobilização da luta contra a SIDA a um maior número de parceiros, alertando para a necessidade da educação preventiva, que a UNESCO quer levar a um maior número de pessoas e locais através de colaborações públicas e privadas.
Criada em 1997, a Coligação Mundial das Empresas contra a SIDA reúne 200 empresas multinacionais que empregam no total mais de 54 milhões de pessoas e encoraja os seus membros a empreender iniciativas no sentido do combate àquela doença. Estas medidas podem ser de carácter global, mas também local, visando os trabalhadores, as suas famílias e as populações vizinhas.
Satisfeito com o acordo, Koichiro Matsuura sublinhou a importância de ter uma "estratégia multiforme" para combater a SIDA e que "o mundo do trabalho é uma parte importante de toda a acção", refere um comunicado da UNESCO.
Por seu lado, Holbrooke mostrou-se confiante em que esta parceria irá permitir "uma acção mais eficaz da parte das empresas e contribuirá para a integração da educação preventiva contra a SIDA na agenda global".
Exército israelita impede doente com SIDA de entrar em Israel
O exército israelita impediu por três vezes a entrada em Israel, para tratamento, de um palestiniano de Gaza hemofílico e doente de SIDA, apesar de se temer pela sua vida, denunciaram hoje fontes médicas.
O doente, de 20 anos, contaminado pelo vírus da SIDA numa transfusão sanguínea, quando criança, foi regularmente tratado no hospital Tel Hashomer, de Telavive, até à eclosão da Intifada há cinco anos.
Numa petição hoje tornada pública, seis especialistas da SIDA fazem saber que a sensível deterioração do estado de saúde do jovem nas últimas semanas torna indispensável a sua admissão no Tel Hashomer.
"O seu sistema imunitário é totalmente deficiente. É um caso patente de necessidade urgente de tratamento", afirma Zvi Bentwich, fundador da primeira clínica israelita para doentes de SIDA.
Os três pedidos feitos neste sentido às autoridades militares israelitas desde 19 de Dezembro foram rejeitados, assinala-se na petição, assinada igualmente pela organização Physicians for Human Rights-Israel (Médicos pelos direitos humanos-Israel).
segunda-feira, janeiro 16, 2006
Brasil lidera coalição para negociar preços
Representatives from 19 Latin American and Caribbean nations said Saturday the countries will act as a bloc to try to reduce the price of AIDS medication, Brazil's official news agency said.
The countries also said they would invest together and exchange information to begin producing the drugs themselves.
The announcement was made after a three-day meeting in Brasilia aimed at discussing regional AIDS prevention. The conference's final report will be presented at the U.N.'s General Assembly in May.
"It's fundamental the countries unite ... to build effective mechanisms to produce medication locally," said Pedro Chequer, the head of Brazil's AIDS program. "The sole negotiation of price reduction won't guarantee sustainability in the long term."
The final report is expected to recommend the creation of methods to measure access to AIDS prevention and treatment, the Agencia Brasil said. The countries also will call for the help of the international community to overcome political and economical barriers in price negotiations.
In recent years, Brazil has negotiated lower AIDS drug prices by threatening to break patents, without ever actually doing so. Last October, after just such a threat, Brazil reached a deal with Illinois-based Abbott Laboratories Inc. to lower the price on the AIDS drug Kaletra.
Chequer had said at the beginning of the conference that Latin American countries that cannot afford increasingly expensive AIDS medication should consider sidestepping foreign patent holders and manufacture the drugs themselves.
According to World Trade Organization rules, countries can issue licenses to disregard patent rights after negotiating with the patent owners and paying them adequate compensation. Governments that declare a public health emergency can skip the negotiating.
Chequer, who had said earlier in the week that Brazil plans to distribute 1.5 billion condoms in 2006, urged other nations not to ban their use on religious or moral grounds.
Brazil accounts for more than half of all AIDS cases in Latin America and the Caribbean, but the government's aggressive prevention efforts have led to a lower infection rate than many had feared.
quarta-feira, janeiro 11, 2006
Soares sobre SIDA
"Pensamento de Mário Soares sobre:
A atenção à infecção pelo VIH/sida
Extractos da intervenção de Mário Soares na Mesa Redonda “Direitos Humanos, SIDA e Responsabilidade Política” do II SEMINARIO SAUDE E DESENVOLVIMENTO realizado pelo Instituto de Higiene e Medicina Tropical nos dias 8, 9 e 10 de Maio de 2002.
REALIZAÇÕES no âmbito da resposta ao VIH/sida
“Como o Professor Jorge Torgal referiu, tive a ocasião de vos receber, enquanto Presidente da República, junto com o Dr. Michael Merson, então Director do Programa Mundial sobre SIDA e a Professora Odete Ferreira, quando dirigia a Comissão Nacional de Luta contra a SIDA.”
“Fiz uma intervenção pública, dizem que a primeira de um Chefe de Estado europeu, em 1994, através da televisão, quando me pediram para dirigir uma mensagem no dia 1 de Dezembro a chamar a atenção dos portugueses para a SIDA”
“ Produzi um texto sobre a problemática da SIDA para o catálogo de uma exposição organizada pela associação Abraço, onde colocava algumas questões que creio serem ainda hoje pertinentes, caracterizando a problemática que esta pandemia nos coloca e que exige a atenção e a responsabilidade política dos Estados.”
“Já fora das minhas responsabilidades como Presidente da República, na condição de Deputado do Parlamento Europeu, comecei a preparar, com o apoio do Dr. Peter Piot, Director Executivo da ONUSIDA, uma sessão Especial sobre o VIH/sida no Parlamento Europeu que espero poder concretizar - se em breve”
“Na qualidade de Presidente da Fundação Portugal - África , uma fundação voltada para o apoio aos países africanos de língua oficial portuguesa, promovi o apoio ao programa REDEsida, que reúne e dissemina informação sobre a SIDA, em língua portuguesa, e contribui para programas de prevenção com a elaboração de folhetos, manuais e outro tipo de meios de informação sobre o VIH/sida que são produzidos com a participação das pessoas ao nível da comunidade , uma metodologia que me parece exemplar nesta área”.
PENSAMENTO SOBRE A INFECÇÃO PELO VIH/sida
“ Defendo que é moralmente injusto e, portanto, inaceitável quer no plano político ou ético, que pessoas, pelo simples facto de estarem infectadas ou afectadas pela SIDA - que não é transmissível nos contactos sociais! - sejam discriminados e lesados nos seus direitos”.
“Não há dúvida que o primeiro dos Direitos Humanos, seja qual for a teoria dos Direitos Humanos, é o direito à vida. E nem que fosse só por esta razão, a prevenção, o acesso aos serviços e aos medicamentos antiretrovirais, que permitem encarar hoje a SIDA como uma doença crónica, têm que ser encarados como componentes do exercício pleno dos Direitos Humanos”.
“As pessoas que vivem com o VIH e com SIDA foram corajosas e inovadoras. Organizaram-se, conquistando a legitimidade do seu conhecimento empirico sobre a infecção, quando antes os doentes eram apenas receptores da autoridade médica. São, por estas razões, reconhecidos parceiros na definição das políticas de prevenção, tratamento e cuidados em vários países. Portugal tem, também, que incorporar a sua voz de um modo, de facto, efectivo”.
“O VIH/sida ao atingir a população mais jovem - mais produtiva e na idade reprodutiva - tornou-se um “problema de segurança nacional” com repercussões económicas, políticas e sociais muito graves que provocam desequilíbrios nos Estados e, até, em certas regiões do mundo. Aqui surge a responsabilidade dos Estados e das organizações de Estados - quer a União Europeia, no nosso caso, quer a OUA e a CPLP no caso dos países africanos - para a que é hoje a mais grave ameaça global à vida humana”.
“É indispensável que os Estados e a Comunidade Internacional realizem um trabalho consertado para garantir o acesso a informação e serviços adequados às distintas condições económicas, sociais, culturais, de género e opção sexual, de modo a favorecer atitudes e comportamentos mais seguros e responsáveis. Temos que trabalhar para manter a esperança”.
CONTEM COMIGO! VAMOS CONSEGUIR! "
Tibotec procura aprovação da EMEA para TMC114
11-01-2006 14:30CORK, Ireland, January 11 /PRNewswire/ ---
Follows Recent Submission of New Drug Application to the US FDA
Tibotec Pharmaceuticals Ltd. announced today that it has submitted an application for marketing authorisation for TMC114, an investigational protease inhibitor for the treatment of HIV-1 infected patients, to the European Agency for the Evaluation of Medicinal Products (EMEA). This submission was completed one week after the submission of a New Drug Application for TMC114 to the United States Food and Drug Administration, which the company announced in December.
Both submissions are based on the efficacy and safety results of the 24-week dose-finding phase of two Phase IIb randomized controlled studies, known as POWER 1 and POWER 2, and supportive data from a non-randomized open label trial, POWER 3. Based on the data from these studies, the submissions to the FDA and EMEA recommend a dose of 600 mg of TMC114 boosted with 100 mg ritonavir twice daily for treatment-experienced patients.
The POWER 1 data were presented at the International AIDS Society (IAS) conference in Rio de Janeiro in July 2005; the POWER 2 data were presented at the 45th Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC) in December 2005 in Washington D.C. Both studies were randomized trials of TMC114 boosted with ritonavir (TMC114/r) in patients with experience of at least 1 PI, 1 NNRTI and 1 NRTI and who had 1 or more primary PI mutations. Patients were randomized to receive optimized background regimen (OBR) plus one of four doses of TMC114/r (400mg/100mg QD; 800mg/100mg QD; 400mg/100mg BID; 600mg/100mg BID) or OBR plus investigator-selected control PI(s).
The POWER 1 results showed that 77% of patients achieved a reduction in viral load (plasma HIV RNA) of 1 log10 or more in the highest TMC114/r dose group, 600mg/100mg BID, compared to 25% in the control group. The most common treatment-emergent adverse events (AEs) in the TMC114/r arms were headache (17%) and diarrhea (16%) compared with 24% and 29% respectively in the control arm. Overall, 14% of both TMC114/r and control patients reported at least one serious AE (SAE).
In patients with more advanced disease, the POWER 2 results showed that 62% of patients achieved a reduction in viral load (plasma HIV RNA) of 1 log10 or more in the highest TMC114/r dose group, 600mg/100mg BID, compared to 14% in the control group. The most common treatment-emergent AEs were headache and nausea, which were each 17% across all TMC114/r arms compared with 17% and 9% respectively in the control arm. Overall, 15% of TMC114/r and 8% of control patients reported at least one SAE.
TMC114, boosted with low-dose ritonavir, is currently in pivotal Phase III clinical trials in both treatment-experienced and treatment-naïve HIV-1 infected patients. The TMC114-C214 trial, for moderately treatment-experienced patients, is investigating a dose of 600 mg of TMC114 boosted with 100 mg of ritonavir twice daily. The TMC114-211 trial, for treatment-naïve patients, is currently recruiting; the study will investigate a dose of 800 mg of TMC114 boosted with 100 mg of ritonavir once daily.
Pending regulatory approval, Tibotec Therapeutics will commercialize the product in the U.S. and Tibotec, a division of Janssen-Cilag, will commercialize the product in Europe and other countries. The trade name for the marketed product has not yet been determined.
Hospitais SA são mais eficientes do que as unidades públicas
Público 11.01.06
A evolução da qualidade e da eficiência dos 31 hospitais com gestão empresarial foi superior à das unidades que mantiveram o estatuto público, revela um estudo da Comissão para a Avaliação dos Hospitais Sociedade Anónima (SA).
A comissão, presidida pelo investigador Miguel Gouveia e criada pelo Ministério da Saúde, pretendeu avaliar o desempenho das 31 unidades do Serviço Nacional de Saúde transformadas em sociedades anónimas em 2002 e que, desde 1 de Janeiro deste ano, viram o seu estatuto jurídico alterado pelo actual Governo, para Entidades Públicas Empresariais (EPE).
(...)
Estudo SMART descontinuado

O estudo SMART estava a decorrer nos seguintes hospitais:
- Hospital Curry Cabral
- Hospital de Cascais
- Hospital de Egas Moniz
- Hospital de Santa Maria
- Hospital Joaquim Urbano
- Hospital São João
11.01.06
Simon Collins
Editor, HIV Treatment Bulletin
The Steering committee for the SMART study have decided to stop further recruitment for the SMART study due to futility, and that people on the treatment interruption arm will receive recommendations to restart treatment.
Although the trials Data and Safety Monitoring Board (DSMB) agreed in November that the study was safe to continue, a more recent review of the data showed a statistically significant difference in AIDS events between the continuous treatment arm and the treatment interruption arm.
The DSMB made a recommendation to stop the study, and the steering committee, after reviewing the unblinded dataset at a meeting in Australia, have agreed to follow this recommendation this morning.
I don't have any further details about these events - whether they are mild (candida etc), or arise from protocol violations (failure to restart when CD4 count falls <250>- further recruitment is stopped from today
- data will continue to be collected
- patients in the discontinuation arm who are currently off-treatment will be recommended to restart treatment.
This final point is the most immediate practical issue, as many patients may be stable and well off-treatment, maintaining a high CD4 count that is well above the trials determined protocol for restarting treatment, and may want to make a personal decision not to restart treatment.
One of the first messages that is also likely to be widely circulated, and which has a huge commercial impact for the pharmaceutical industry is that 'treatment is for life'. Although none of the data has been released yet, I find this aspect most depressing, and think that this would be the wrong interpretation from the decision that has been made to stop the study.
It is clearly disappointing that this study, planned as the largest and one of the longest running studies, that also has a high level of support in the community, is being stopped before recruitment was even completed, after only 2 of the planned 9 years follow-up.
However everything is in the details of the study results. It may be that the study answer has been reached much earlier than expected, and the benefits of continued treatment clearly outweigh any use of treatment interruption. Or it may be that the original study assumptions did not match actual reported events and that the study design itself can't answer the original question.
Relato dos protestos na Tailândia

{kind=link}
Gaëlle Krikorian, a participant in the protests working with Thai AIDS activists, described the situation this way:
"Today, about 8,000 people were demonstrating in Chiang Mai. In front of the Sheraton hotel, people were demanding that the negotiating teams send representatives to tell them what exactly they are negotiating. Nit Pibulsongkram, the head of the Thainegotiating team came out surrounded by police and said that this is the wish of the 'elected government' to do this agreement for the benefit of the country. People trying to enter the hotel were beaten by the police. 30 people tried to swim across the river to reach the hotel and were beaten too."
Protestos na Tailândia contra negociações comerciais

Reuters 10.01.06
Thousands Protest Against U.S.-Thai Trade Talks
by Sukree Sukplang
Thousands of Thais marched through the northern city of Chiang Mai on Monday to protest against a U.S.-Thai free-trade pact as officials began a sixth round of negotiations.
The protesters, including farmers from the drought-plagued northeast and HIV/AIDS patients in Bangkok, marched 2 km (1 mile) from the city's main train station to the U.S. consulate chanting and waving placards.
"We want the whole negotiation process to end because they are not transparent and against the constitution," said Kannikar Kittivechakul of the People's Network Against Free Trade Agreements and Privatization's, which organized the rally. The group said a free-trade pact would result in the privatization of public utilities under U.S. management and farmers would suffer from cheap farm imports while paying more for U.S.-made drugs.
The United States is Thailand's largest trade partner. Thai exports were worth $15 billion in 2004 and imports $7.2 billion. Neena Moorjani, spokeswoman for the U.S. trade delegation, called the protests "a sign of healthy democracy."
Trade negotiators resumed talks on Monday. A Thai negotiator said last week services and financial sectors, left aside in early rounds, would be on the table during the week-long meeting.
Pharmaceuticals, another delicate issue, were also likely to be discussed despite opposition from groups that fear Thailand's generic drug industry would be hurt, Thai chief negotiator Nitya Pibulsonggram said.
William Aldis, the World Health Organization representative in Bangkok, said Thailand should think carefully about surrendering access to cheap medicine in exchange for a free-trade deal. "The stakes are indeed high, especially for the 600,000 Thais living with HIV/AIDS and whose survival will depend on the availability of affordable anti-retroviral drugs," Aldis wrote in the Bangkok Post newspaper.
Moorjani said the U.S. delegation hoped a final deal could be wrapped up in a few months.
"Specifically, we hope to make sufficient progress on the text of the chapters under negotiation as well as market access," she said in a statement to Reuters.
GAT manda carta à embaixada americana
Embaixada dos Estados Unidos da América
Av. das Forças Armadas
1600-081 Lisboa
Lisboa, 9 de Janeiro de 2006.
International NGO Solidarity Statement: US-Thai Free Trade Negotiations Threaten Access to Medicines; Activists Demand Suspension of Negotiations and End to TRIPS-plus IP Provisions
Thai AIDS activists and their international allies are seeking suspension of scheduled trade talks that threaten to undermine Thailand¹s lawful ability to produce, import/export, and market low-cost generic versions of life-saving medicines. Today, in Chiang Mai, the United States and Thailand are scheduled to start the Sixth Round of negotiations on a proposed Free Trade Agreement and for the first time are holdingdiscussions on a U.S. proposal to dramatically increase intellectual property protections for pharmaceutical products. Simultaneously, ten thousand Thai activists, half of them living with HIV, are protesting the scheduled talks and trying to shut them down, promising to sleep overnight outside the meeting venue for three nights and to block entry to the negotiations.
The U.S. government has consistently refused to release the draft text ofits FTA proposals and simultaneously extracts promises of secrecy from itsnegotiating partners. This shroud of secrecy limits democratic review andcivil society participation in the negotiation process. In particular, it denies voice to the tens of thousands of Thais living with HIV/AIDS who need increased access to affordable second-generation antiretroviral and opportunistic infection medicines that are currently patent-protected and cost prohibitive.
Instead of allowing Thailand to use all existing flexibilities for accessingcheaper medicines under international law as confirmed by the 2001 WTO Doha Declaration on the TRIPS Agreement and Public Health and by the UNCommission on Human Rights, the U.S., based on past practice, will be seeking to heighten patent and data protection in the following ways:
- Extending patent terms beyond 20 years to compensate for administrative delays and easing standards of patentability on new formulations and uses, thereby extending the period of monopoly pricing;
- Restricting rights to parallel import cheaper medicines by codifying patent-holders¹ rights to contractually limit export/import of previously sold products;
- Potentially restricting the grounds for issuing compulsory licenses;
- Linking marketing approval to the absence of claimed patent rights and imposing 5-10 year data-exclusivity provisions (preventing reliance on proprietors¹ clinical trial data to grant marketing approval for generic products), thereby potentially restricting compulsory licensing rights;
- Imposing criminal penalties on companies that intentionally or inadvertently violate patents.
The U.S. attempts to down-play the significance of these hard-text treatyterms with an ambiguous and under-inclusive "side-letter" reaffirming tradepartners¹ rights to prioritize access to medicines. Such side-letters make no binding commitments, and the USTR has expressly declined to confirm the obligatory effect of the letters when asked to do so in response to Congressional inquiries.
Consistent with human rights norms requiring access to essential medicinesand in response to Thai activist demands, Thailand has initiated a programof universal access to government-subsidized antiretroviral drugs that nowreaches 70,000 of 170,000 Thai people living with HIV/AIDS. However, the future costs of expanded treatment with newer patented medicines will beprohibitive if the U.S. succeeds in its objectives to ratchet-up intellectual property protections.
Therefore, G.A.T.- Grupo Português de Activistas sobre Tratamentos de VIH/SIDA-Pedro Santos joins its Thai colleagues at Chiang Mai and throughout Thailand demanding that the U.S. suspend negotiations on intellectual property rights and that it drop all intellectual property provisions affecting access to pharmaceutical products, specifically all TRIPS-plus terms, in the Thai FTA and in other FTAs as well. In addition, we demand that the U.S. publish its proposed text for the entire FTA and that the Thai people have had a chance to hold public consultations on the proposed agreement.
Yours sincerely,
G.A.T.- Grupo Português de Activistas sobre Tratamentos de VIH/SIDA-Pedro Santos
segunda-feira, janeiro 09, 2006
Seringas nas prisões à espera de novo estudo

Governo nomeia grupo para apresentar propostas em seis meses
DN 06.01.06
A introdução de troca de seringas nas prisões - à semelhança do que é feito para os toxicodependentes fora do meio prisional - está dependente de um novo estudo. Ontem, os ministros da Saúde e da Justiça nomearam um grupo de trabalho que tem seis meses para apresentar propostas concretas nesta matéria.
O despacho governamental surge na véspera de os grupos parlamentares do BE e de "Os Verdes" levarem à votação na Assembleia projectos-lei para aplicar esta medida, que consideram urgente devido às altas taxas de infecção por HIV/sida ou hepatites. Num estudo a decorrer em duas penitenciárias, a prevalência de HIV chega aos 10% e a de hepatite C aos 15%.
Recorde-se que há dez anos que o PS defende a redução de danos dentro das prisões (ver texto ao lado). Contudo, as medidas continuam por aplicar. Mas para o ministro da Justiça, Alberto Costa, "este é um novo Governo, portanto tem de fazer a sua própria avaliação". Considera que "as questões de segurança são decisivas mas se o estudo for concludente não há qualquer preconceito".
"Não quero acreditar que o PS está a vacilar." O deputado de "Os Verdes", Francisco Madeira Lopes, diz esperar que a criação do grupo "não seja um pretexto para inviabilizar a troca de seringas" e que "se estudem outras intervenções".
Já o presidente do Instituto da Droga e da Toxicodependência (IDT), João Goulão, atribuindo aos dois partidos "o mérito de terem desencadeado este processo", crê que "o despacho governamental é um sinal de comprometimento político e que já não há retorno".
Goulão admite até que "as conclusões cheguem antes do prazo de seis meses". Por saber, estão as modalidades que serão adoptadas - máquinas de troca de seringas ou salas de injecção assistida. Resta outra questão a montante definir qual dos ministérios (Saúde ou Justiça) fica com a tutela da saúde dos reclusos. "Há zonas de penumbra, como se cada ministério estivesse a fazer cerimónia com o outro. E definir competências é uma forma de responsabilização", diz o responsável pelo IDT, para quem "deverá ser a Saúde" a assumir o sector. Sobre a necessidade de ser feita uma nova análise, quando existem já estudos conhecidos, refere que "há um conjunto de medidas que têm enfrentado tradicionais resistências".
As duas objecções clássicas à introdução do programa de troca de seringas nas prisões são a admissão da entrada de estupefacientes ilegais e o receio de que as seringas possam ser usadas pelos reclusos como armas. O primeiro argumento tem sido progressivamente abandonado, face à evidência - no já citado estudo, 39,7% dos reclusos admitiram ter consumido haxixe e 3% heroína nos últimos 30 dias. E os próprios representantes dos guardas prisionais admitem o facto "Ninguém pode negar que entra droga."
A razão pela qual o Sindicato dos Guardas Prisionais se opõe à troca de seringas são os "problemas de segurança". "No dia em que entrarem seringas nas cadeias não entram os guardas prisionais", assevera o vice-presidente, Ramiro Fernandes. Contudo, admite não conhecer as experiências internacionais, nomeadamente em Espanha, onde o programa existe em mais de 30 prisões. "Não estou inteiramente dentro do assunto para discutir isso." E assume que uma fórmula que não entregue seringas aos presos "para ficarem com elas", como as salas de consumo assistido, poderia obter a concordância dos guardas.
Tribunal recusa indemnização a homem infectado no Hospital de Santo António
Público 05.01.06
O Supremo Tribunal Administrativo recusou o pagamento de uma indemnização a um homem que contraiu o vírus HIV2 durante uma transfusão de sangue, em 1986, no Hospital de Santo António, no Porto, avança a edição de hoje do "Diário de Notícias".
De acordo com o DN, num acórdão de 14 de Dezembro passado, os juízes admitem que, entre 1975 e 1987, o Hospital de Santo António recebeu sangue de um dador infectado com o HIV2. O vírus HIV2 e HIV1 (vírus da imunodeficiência humana) estão na origem da sida (síndroma da imunodeficiência adquirida) e pertencem à mesma família, apesar de serem diferentes geneticamente.
Os juízes do Supremo consideraram, no entanto, que naqueles anos a despistagem do vírus ainda não era possível e que as transfusões de sangue não são uma actividade "excepcionalmente perigosa". O caso remonta a 1986, quando Joaquim Conceição, nascido em 1942, recorreu ao Hospital de Santo António para uma intervenção cirúrgica em ortopedia, em consequência de vários trabalhos na marinha mercante, e que implicou uma transfusão de sangue.
Em 1990, Joaquim Conceição foi diagnosticado como portador do vírus HIV2 e a explicação para o facto viria a ser conhecida quatro anos mais tarde. Segundo o jornal, os responsáveis hospitalares admitiram que, durante 12 anos - entre 1975 e 1987 -, tiveram um dador de sangue portador daquele vírus, que foi identificado apenas em 1987, quando a despistagem começou a ser possível.
Em 1994, Joaquim Conceição (que morreu em 2001) resolveu, juntamente com a companheira, intentar uma acção contra o hospital e contra o Estado, com vista à condenação destes ao pagamento de uma indemnização. Os acusados consideraram o caso prescrito e o Estado - representado pelo Ministério Público - alegou ser parte ilegítima, desviando as responsabilidades para o hospital.
A questão chegou ao Supremo Tribunal Administrativo (STA) que, em 2000, deu razão ao Estado, considerando que este nada tinha a ver com o assunto, sem admitir, no entanto, a prescrição do processo. O caso foi então julgado no Tribunal Administrativo e Fiscal (TAF) do Porto, em 2004, tendo como réu apenas o hospital. O juiz do TAF conclui que não houve qualquer acto ilícito ou culposo por parte dos técnicos de saúde, salientando que só a partir de 1987 foi possível despistar o HIV2. O hospital foi absolvido. Mas o advogado de Joaquim Conceição, Lázaro Ferreira, recorreu da decisão para o STA, que, a 14 de Dezembro último, confirmou a sentença anterior. O advogado considerou esta decisão "indigna de um Estado de direito".
Lázaro Ferreira disse ao DN que ficou "incrédulo" e acrescentou que "desde o início dos anos 80 que vários países europeus, como a França, a Inglaterra ou Alemanha, se disponibilizaram para indemnizar todos os contaminados por transfusões sanguíneas". De acordo com o DN, o Supremo Tribunal Administrativo decidiu de modo oposto numa outra sentença, em Março de 2005, estabelecendo a perigosidade das transfusões de sangue e condenando o Hospital de Cascais a indemnizar uma paciente infectada com HIV1. No caso desta paciente a transfusão foi feita em 1994, numa altura em que já se fazia a despistagem.
Acesso universal em 2010?
AIDS Treatment Activists Call on the U.N. and National Governments to Fulfill the Promise of the G8 Universal Access Goal
NEW YORK, Jan. 6 /U.S. Newswire/ --
On the eve of a meeting of U.N. officials, representatives of national governments and civil society to outline a plan for achieving the G8's goal of near universal access to AIDS treatment, the International Treatment Preparedness Coalition (ITPC) today called on multilateral organizations and national governments to lay concrete plans to realize the G8 goal by 2010. ITPC is a network of over 600 people living with HIV/AIDS and their advocates from over 100 countries.
In November 2005, ITPC released a detailed report on the failure to meet the World Health Organization's "3 by 5" goal. (The report, Missing the Target: A Report on HIV/AIDS Treatment Access from the Frontlines, is available at http://releases.usnewswire.com/redir.asp?ReleaseID=58923&Link=http://www.aidstreatmentaccess.org ).
In December 2003, the World Health Organization made a commitment to extend AIDS treatment to three million people in the developing world desperately in need of therapy by 2005. By the end of last year, the international community, U.N. agencies and national governments had fallen short of that goal by over one million people.
At their summit in 2005, the G8 set an even more ambitious goal of coming as close to possible to universal access to AIDS treatment by 2010. This year, the Joint United Nations Programme on AIDS (UNAIDS) and the Department of International Development of the United Kingdom (DFID) are leading an effort to implement universal access. In Washington, D.C., next week, leaders from around the world will converge to outline the plan for achieving the G8 goal.
"Millions of lives depend on the outcomes of meetings such as this. As we come together to begin to plan for universal access, we cannot allow politics or bureaucracy to sideline us from our goal. Without a well-defined, task-oriented approach to the implementation of the Universal Access initiative, the effort is likely to be another in a series of hollow promises to people living with HIV/AIDS from the U.N. and governments around the world," said Rodrigo Pascal, co-chair of the International Steering Group of the ITPC.
ITPC calls upon UNAIDS and DFID to ensure:
1. The Universal Access initiative sets clearly-defined, iterative, and measurable goals to frame treatment scale up efforts, including quarterly national and international targets for access to treatment.
2. Specific goals, objectives and tasks be set for national governments, multilateral agencies, and others.
3. Meetings of the Global Steering Committee that is planning the Universal Access initiative focus on practical issues involved in scale up, including improved technical assistance and support to address specific barriers such as procurement, supply chain management, programme management, and planning.
4. Progress on these objectives be readily transparent.
5. Funding from donors be contingent on progress towards the agreed upon goals, objectives and tasks. Outcome-based incentives should be established on the country, regional and international levels to support the initiative.
6. The resources of multilateral and bi-lateral agencies be utilized in a more efficient, strategic approach to addressing challenges on the country level. An inventory of resources should be established by the international community to aid in treatment and prevention scale up.
7. Creation of a multilateral mechanism to troubleshoot and resolve challenges on an ongoing basis.
ITPC will continue to monitor treatment scale up efforts on the national and international levels. The group plans to issue updates to its treatment report over the coming months.
---
The International Treatment Preparedness Coalition (ITPC) was born at the International Treatment Preparedness Summit that took place in Cape Town, South Africa in March 2003. That meeting brought together for the first time community-based treatment activists and educators from over 60 countries. Since the Summit, ITPC has grown to include over 600 activists from around the world and has emerged as a leading civil society coalition on treatment preparedness and access issues.
sexta-feira, janeiro 06, 2006
Moçambique precisa de 15 ME para combater a SIDA
O Conselho Nacional de Combate à SIDA (CNCS) de Moçambique necessita este ano de 15 milhões de euros para desenvolver acções de luta contra a doença no país, disse hoje à Agência Lusa a directora executiva da instituição.
O montante servirá para a realização de diversas actividades de combate ao SIDA, designadamente a prevenção, mitigação, investigação e tratamento, que irá incidir sobretudo à zona centro, região mais afectada pela doença, referiu Joana Mangueira.
Dados oficiais indicam que 16 por cento da população adulta de Moçambique (entre os 15 e 49 anos) está infectada pelo HIV, vírus que causa a SIDA, enquanto a região centro do país conta com uma taxa de infecção superior a 25 por cento.
Segundo as autoridades moçambicanas, 95 por cento dos casos de infecção por vírus resultam de relações sexuais desprotegidas, facto relacionado com questões de índole cultural. Este ano, "o trabalho de prevenção deverá tomar em consideração a realidade sócio-cultural de cada região do país, para qualquer projecto de intervenção na área da SIDA", assinalou a responsável do CNCS.
"Vamos trabalhar com mapeamento que cada província está desenhar, que deverá destacar como grupo alvo a mulher e a criança", acrescentou. O governo moçambicano pretende ainda um maior envolvimento dos líderes comunitários e outras personalidades influentes nas zonas rurais no combate à doença, devendo "consolidar o trabalho de prevenção das crianças nas escolas", destacou Magueira.
"Queremos que a escola se torne um centro de habilidades para a criança de forma a preveni-la da doença. O nosso principal desafio é a mudança de atitude", sublinhou a secretária executiva do CNCS.
O CNCS admite reforçar o montante, para permitir uma melhor intervenção da sociedade civil moçambicana, concluiu.
Angola - 3.587 novos casos de SIDA entre Janeiro e Outubro
As autoridades sanitárias angolanas registaram 3.587 novos casos de SIDA no país entre Janeiro e Outubro de 2005, o que representa um aumento de "mais de 20 por cento" em relação a igual período do ano anterior.
Os dados foram hoje revelados à Agência Lusa por Dulcelina Serrano, directora do Instituto Nacional de Luta contra a SIDA, acrescentando que já foram diagnosticados 19.196 casos desta doença em Angola desde 1985, altura em que foi registado o primeiro caso no país.
Segundo Dulcelina Serrano, "todo o país foi tocado pela epidemia, mas a maior prevalência ocorre nas províncias de Cabinda, Cunene, Lunda Norte, Lunda Sul, Uíge e Cuando Cubango, que fazem fronteira com países onde existe um elevado nível de prevalência da doença". A província de Luanda também apresenta um dos níveis mais elevados de prevalência da SIDA em Angola, devido às suas "características especiais" enquanto capital do país.
A directora do instituto adiantou, por outro lado, que a transmissão da doença por via sexual continua a ser a principal causa de propagação, sendo responsável por "mais de metade dos casos notificados".
Relativamente ao tratamento com anti-retrovirais, Dulcelina Serrano salientou que actualmente estes medicamentos estão disponíveis apenas em cinco províncias, mas frisou que "até Setembro será coberto todo o país". Os anti-retrovirais estão actualmente disponíveis apenas nas províncias de Luanda, Cunene, Cabinda, Huíla e Uíge.
No início de Novembro, a ONUSIDA, agência das Nações Unidas para o combate à doença, admitiu que a SIDA poderá ser responsável, em 2010, pela existência de mais de 330 mil crianças órfãs em Angola.
Segundo os dados da ONUSIDA, em 2001, a doença foi responsável por cerca de 15 por cento dos órfãos em Angola, percentagem que ultrapassou 20 por cento no final de 2005 e deverá atingir 34 por cento em 2010.
As autoridades angolanas estimam que perto de cinco por cento dos cerca de 13 milhões de angolanos que vivem no país estejam infectados com o vírus da SIDA, sendo o combate à esta doença uma das prioridades nacionais em termos de saúde pública.
Angola possui a mais baixa taxa de prevalência de SIDA entre os países da região da África Austral, mas vários responsáveis do sistema das Nações Unidas têm vindo a alertar para a necessidade de adoptar medidas que permitam aproveitar esta situação para combater o alastramento da doença.
terça-feira, janeiro 03, 2006
Comissão Europeia sobre SIDA
O fim de 3x5
GMHC
23 de Dezembro de 2005
What we're seeing now is the "return of the repressed," that is, instead of an activist WHO under Bernhard Schwartlander (who came up with 3x5) and Jim Kim (who implemented it), we're getting a public health traditionalist at the helm of the organization, Kevin DeCock, sometime in March (the interregnum, where the HIV/AIDS Department sits headless is notable in itself in terms of indicating the importance or lack of it that HIV/AIDS really enjoys at WHO).
I think it's fair to call Kevin a traditionalist, as he invokes Thomas Parran, US Surgeon General under US President Franklin D Roosevelt and Parran's book, Shadow on the Land, published in 1937, in which the Surgeon General outlined his plan to combat syphilis, as a clear model for himself as he muses about AIDS in Africa, in his famous 2002 Lancet article, Shadow on the Continent.
We are also seeing a return of the Blob of the WHO's bureaucracy, which like the star of the eponymous 1950s horror flick, consumes everything in its path, turning programs into jelly.
Let's be clear: 3x5 wouldn't have happened without the groundswell of grassroots support for treatment access from the Treatment Action Campaign, from HealthGAP, from MSF, from many, many other groups outside the mainstream of global public health.
Now, we have G-8 leaders, mostly the English, and UNAIDS trying to placate the outsiders, by telling us, 3x5 isn't over, it's now Universal Access by 2010. This would have been a credible sequel to the 3x5 initiative if some new goals had been announced with an analysis of why the previous effort failed to achieve its own targets and a call for us all to move ahead together with a spirit of renewed purpose and determination.
What we've seen instead is that Universal Access by 2010 is universal access to HIV treatment, care, prevention, human rights, stigma reduction, etc.---yes, it's heaven on earth in four years' time and I have nothing to wear to the party!
Moreover, there will be no "global" targets for the new Universal Access Initiative, which is to be country-driven. Of course, there will be no global targets. Global targets are scary. Eeek! The UN system, bilaterals, national governments get judged on outcomes with global targets. Targets might have to come with a plan to achieve these goals, with milestones and timelines. How much better to sit in Geneva and not have to feel responsible for reaching any target---whew, I have a lovely, well-paying job, in a lovely city by the lake, I already sweat enough during the summer here to have to sweat and worry all year round about reaching millions of people with AIDS treatment by 2010, 3x5 was bad enough...
And countries, yes, the countries, which complained loudly about targets in the first place: how dare anyone suggest to sovereign nations that they actually should try to treat 50% of their citizens dying from a treatable disease, it's outrageous. Only death will separate African politicians and elites from their Mercedes. In East Africa, they are called the wabenzi — men of Mercedes Benz — in Swahili, writes George Ayittey, in his Africa Unchained: The Blueprint for Africa’s Future. Only HIV/AIDS (tuberculosis, malaria) will separate African children from their parents, parents from their babies, husbands from their wives, wives from their husbands. So, let's see what 2006 brings.
Perhaps, I am too cynical and this series of meetings both on the international and country level on universal access will bring us detailed plans of actions, with specific measureable goals, milestones and timelines (e.g. 3 million on treatment by 2006, 4 million by 2007, 6 million by 2008....). I doubt it -we're slipping backwards in time now- on December 1st of this year, while our brave colleagues in Zimbabwe were getting thrown into jail for daring to demonstrate about access to treatment and the rights of people living with HIV/AIDS, back in Geneva, 3x5 was getting airbrushed out of the UN agencies' World AIDS Day festivities.
How different is this from 2000, when in Durban at the AIDS conference, the Treatment Action Campaign began to galvanize the world about the right to treatment. Zackie Achmat was once talked about for a Nobel Prize, but this December, it's Bill "I don't do treatment, I do prevention, and sometimes shiny new health toys" Gates and U2's ''drop the debt" Bono on the cover of Time magazine... HIV/AIDS is getting "mainstreamed to death" now--AIDS, everything about it, is being put into a big pot called All the World's Troubles, in which it's hard to pick out individual issues at all anymore, let alone organize a response to them.
Yet millions of consultants and officials (some rich men and rock stars) stand around the pot having meetings, giving a big stir to the pot once in a while to show they are earning their salaries or their accolades. When we say something, they remind us they are the experts, they are our leaders, and if we insist on claiming our rights, they dump us in a prison in Harare, Douala, Kaliningrad....
I think I know what we have to do in 2006-as labor organizer Joe Hill said as he was being put to death in the USA many years ago, he said, "don't mourn, organize." Well, we need to organize. Let's stop trying to out-expert-the-experts, showing them we know as much as they about diagnostics, health systems, intellectual property, procurement, tuberculosis. Let's politically organize wherever and whenever we can and help our colleagues in other countries to do so. This isn't about meetings and reports, this is about organizing a world-wide political campaign, with messages and media, a level of discipline and coordination that other successful political campaigns have had.
Most people I know now aren't doing political work, if they are, they are not in the USA, where we meet with each other and our opponents, where we criticize them and they criticize us, but unlike them, we have no political base of power any longer in the USA, we are talking heads without bodies. The advances we did secure early in the epidemic in this country were when there were people on the streets in San Francisco, New York, thousands of people, not dozens or hundreds, and millions marched on Washington to demand our rights.
So, it's time to go back to basics, and many of us remember how to do this, but somehow have drifted away from this kind of work. Yes, it's difficult, in the 1980s and 1990s, this kind of political organizing happened spontaneously and as the movement began to die at the beginning of the first Clinton Administration, we were tired and were all too glad to believe that finally we could get what we want from our leaders.
The Campaign to End AIDS is a noble attempt to revive the activist spirit, but why has it failed to catch fire, pull in significant resources, though it did give hundreds of new people a way to tap into the work. It now has to be brought to scale here in the US, were thousands and millions are demanding our rights once again. If we could put our collective brain-power together to figure out how to bring activism back to scale, well, that would be a critical task.
![]()